![]() Case
Information - Claim
Data
Case
Information - Claim
Data
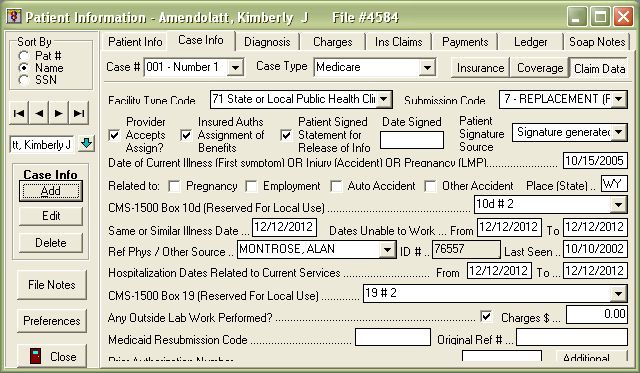
The Claim Data section of the patient's Case Information contains several fields that will map to a printed CMS-1500 insurance claim form or its electronic equivalent. It is not necessary to always fill out all of the fields in Claim Data in order to have your insurance bills accepted. However, certain insurance carrier's have their own requirements as to what is and what isn't required on the claim.
! IMPORTANT: A QuickPractice representative cannot always give you a definitive answer as to what an insurance carrier specifically requires on the claims that you send them. It is the client's responsibility to contact the carrier to confirm what is needed on the claim (such as a "ate of current illness or C.L.E.A. number). After you are sure of what needs to be included on the claims you send, you may always contact a technical support technician to inquire as how to use the program to populate that information to the insurance form.
Refer to the following screenshot and table as a reference for how each field in Claim Data maps to your insurance claims.
|
|
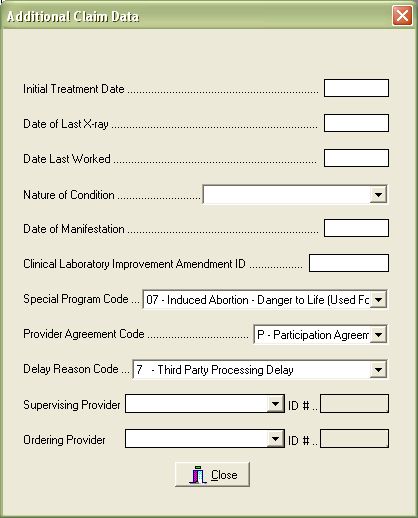
At the bottom of your Claim Data screen you will notice an "Additional" button. Click on this button to view the screen containing fields for less common requirements for electronically submitted insurance claims.
|
Refer to the following screenshot and table as a reference for how each field in Claim Data maps to your insurance claims.
|
|